The Embodied Mind Research Group (EMRG)
A Unified Science of Embodiment: How the Brain Creates the Experience of “Me”
How does your brain know that this body is yours? And what happens when that process goes wrong?
The EMRG studies how the brain builds the experience of being a body. We investigate how we come to feel ownership over our limbs, how we sense internal bodily signals, and how these processes shape mental health and recovery after injury.
Our research connects laboratory experiments, brain science, and clinical work. By understanding the basic mechanisms through which we construct bodily experience, we aim to improve how we understand mental health and neurological conditions.
The EMRG is a highly active research group, with members at institutions spanning three continents:
Dr Pietro Caggiano
Dr Fabio Castro
Dr Aaron Clarke
Dr Daniela Compton
Dr Compton’s research focuses on embodiment and interoception within predictive processing frameworks. She examines how multisensory integration and internal bodily signals contribute to body ownership, belief updating, and behaviour. Her work has a particular focus on clinical and subclinical variations in psychopathology, especially obsessive–compulsive symptoms. She also has a background in philosophy, with prior work on embodied and enactive approaches to emotion and cognition.
Daniel Fray
Daniel Fray’s research focuses on the integration of body and mind, with particular emphasis on how different sensory modalities contribute to perception and body representation. He is interested in how these processes vary in clinical populations and how they are shaped by prior expectations. His work uses behavioural and neurophysiological measures to investigate these mechanisms, with the longer-term aim of developing adaptive technologies that can be integrated into everyday life.
Dr Charlotte Dean
Prof Paul Jenkinson
Prof Jenkinson is Associate Dean of Research at The Cairnmillar Institute (Melbourne, Australia). His research uses a range of methods, including experimental psychology, neuropsychology, multisensory illusions, social, cognitive and affective neuroscience, meta-analysis, and computational modelling. His work aims to understand how the body contributes to everyday experience in both healthy and clinical populations, and to translate these insights into improved approaches to mental health treatment.
Website.
Google Scholar Profile.
Prof Keith Laws
Prof Laws’ research investigates cognitive dysfunction in mental health disorders, particularly schizophrenia and obsessive–compulsive disorder, and how these processes relate to symptom expression and clinical outcomes. A key strand of his work focuses on body representation, interoception, and embodiment, exploring disturbances in bodily experience in psychiatric and neurological conditions. He also specialises in meta-analysis, having led numerous quantitative reviews of mental and physical health interventions to inform evidence-based treatment.
Google Scholar Profile.
Nicholas Lynch
Nicholas Lynch is a PhD researcher in psychology at the University of Hertfordshire. His research focuses on embodiment, interoception, and obsessive–compulsive symptomatology, with a particular interest in predictive coding accounts. His work explores how bodily self-consciousness and internal bodily signal processing relate to both clinical and subclinical obsessive–compulsive experiences.
Jo Mash
Jo Mash’s research explores how perceptual distortions, such as hallucinations and illusions, can reveal the underlying mechanisms of the mind and brain. Her work investigates phenomena such as “strange face” illusions, in which viewing one’s reflection in low light can produce vivid and often unsettling perceptual changes. These experiences provide a unique window into how the brain constructs identity, self-perception, and reality.
Dr Laura Mora
Dr Mora’s research lies at the intersection of neuropsychology and cognitive neuroscience, focusing on how the brain constructs and updates representations of the body. She studies the role of multisensory integration and neuroplasticity in shaping bodily awareness, with particular interest in how these processes can be applied in clinical populations. Her work emphasises translational research, linking experimental findings to outcomes in neurorehabilitation.
Google Scholar Profile.
Dr Valeria Piombino
Dr Piombino is affiliated with Charles University (Faculty of Humanities, Prague) and the National Institute of Mental Health (Czech Republic). Her research focuses on how the brain constructs and maintains body representations, building on earlier work on phantom limb pain and cortical body maps. She now investigates how interoceptive signals interact with pain and perception using experimental and psychophysiological approaches. Drawing on a dual background in cognitive neuroscience and clinical sexology, her work explores the interplay between body awareness, pain, and sexuality in both research and clinical contexts.
Google Scholar Profile.
Dr Diamantis Toutountzidis
Dr Toutountzidis’ research focuses on trauma, psychosis, and crisis mental health, with particular interest in the relationship between early adversity and mental health outcomes. He also works on psychological interventions for psychosis, including trauma-focused approaches, and on service innovation in crisis care, such as Open Dialogue and community-based models.
Google Scholar Profile.
Predictive Processing and Embodied Selfhood
When recognising your body and your face goes wrong
Our research uses multi-sensory illusions to reveal how the brain constructs our sense of self. These illusions demonstrate how the brain combines sensory signals with expectations to generate our experience of who we are. Some examples are:
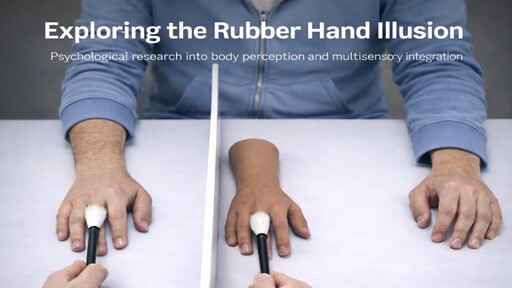
The Rubber Hand Illusion: When Your Body Isn't Quite Yours
When a person's real hand is hidden while a visible rubber hand is stroked simultaneously, many people feel the rubber hand belongs to them - experiencing ownership over an object that isn't their biological body.
This shows that body ownership is not fixed. The brain combines vision, touch, and proprioception to decide what is "me." When signals synchronise, the brain updates its body model - incorporating a false hand or even other objects. When predictions are confirmed (i.e. vision + touch + position align), the brain accepts the rubber hand as "mine."
We examine how susceptibility varies across a range of conditions, including schizophrenia, eating disorders, obsessive compulsive disorder, and autism. Some individuals show strong visual dominance, others rigid proprioceptive priors. These differences reveal how predictive processing mechanisms - precision weighting and representational flexibility - vary across conditions, helping explain distorted body size in eating disorders and alien control experiences in schizophrenia.
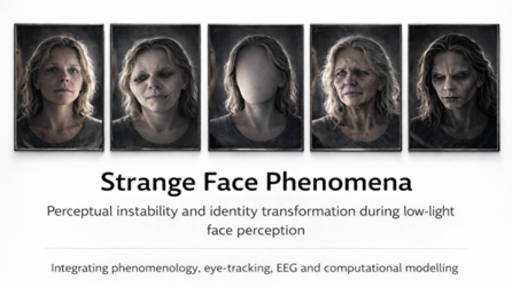
The Strange Face in the Mirror Illusion: When Your Face Becomes a Stranger
When people gaze at their reflection in near-darkness for several minutes, many report vivid experiences, with their face shifting, distorting, or transforming into unfamiliar identities. These Strange Face Phenomena underlie cultural rituals like Bloody Mary, yet reveal how the brain constructs identity.
This illusion shows that facial identity is actively constructed through predictive inference, not simply "read off" visual input. In low light, degraded signals force the brain to rely on predictions and when coupled with staring at one’s own face, this destabilises perception. Under these conditions, predictions dominate, generating hallucinations. This reveals the fragility of self-recognition, which depends on balancing sensory input and expectation.
When people stare at their reflection in very dim lighting, the visual signals from the face become weak and unreliable. In these conditions, the brain begins to rely more heavily on its expectations and prior experiences to “fill in the gaps.” As a result, the face in the mirror can appear to distort, change identity, or even look like someone else entirely. These strange experiences reveal something important about how perception works: our sense of recognising our own face depends on a delicate balance between incoming sensory information and the brain’s predictions. When that balance is disrupted, even something as familiar as our own reflection can become unstable and surprising
We combine phenomenological analysis, eye-tracking, EEG, and computational modelling to investigate how mirror-gazing in low light pushes the brain into a state where predictions overwhelm sensory evidence. Similar experiences appear to occur in depersonalisation, psychosis, body dysmorphic disorder, and eating disorders. We study how perception, expectation, and belief create coherent selfhood, and how predictive disturbances generate illusions and hallucinations.
Interoception
Interoception – The Inner Sense That Shapes the Mind
Interoception is the brain’s perception and interpretation of signals from inside the body, such as your heartbeat, breathing, and sensations from your stomach. These signals form the biological foundation of many psychological processes, such as emotion, motivation, and self-awareness. Every feeling of anxiety, calm, fatigue, or anticipation depends on how the brain detects, interprets, and regulates these internal cues. Our work examines interoception across clinical and non-clinical settings, including eating disorders, depression, anxiety, and obsessive–compulsive disorder (OCD).
Recent Projects
Interoception in Eating Disorders
Our research involving over 4,000 individuals with eating disorders found markedly elevated self-reported interoceptive difficulties across anorexia nervosa, bulimia nervosa, binge eating disorder, and related conditions. Crucially, these differences were also present in individuals who had recovered, suggesting that altered interoception may represent a stable vulnerability factor (endophenotype), and not simply a consequence of acute illness. Our findings indicate that disrupted awareness and interpretation of bodily signals, including hunger, fullness, and emotional states, play a central role in the development and persistence of eating disorders. Interoception therefore represents both a transdiagnostic mechanism and a promising target for assessment and intervention.
Interoception in Depression
In a recent multi-level meta-analysis of 49 studies spanning almost 22,000 participants across 15 countries, we found that depression is not primarily characterised by an inability to detect bodily signals. Instead, difficulties appear to lie in how bodily sensations are interpreted and used. Adaptive body awareness - trusting bodily signals and using them to guide emotional regulation - was consistently associated with lower depression. In contrast, hypervigilant monitoring and catastrophising about normal bodily fluctuations were linked to higher depressive symptoms. These findings suggest that the way we relate to our internal bodily signals, rather than simply how accurately we detect them, is central to our emotional wellbeing.
Interoception in OCD
In ongoing work, we are examining at how interoception might be a core factor in OCD. This work includes a review of existing studies looking at the relationship between interoception and OCD, and new studies examining how interoception might be associated with a broad range of OCD related behaviours.

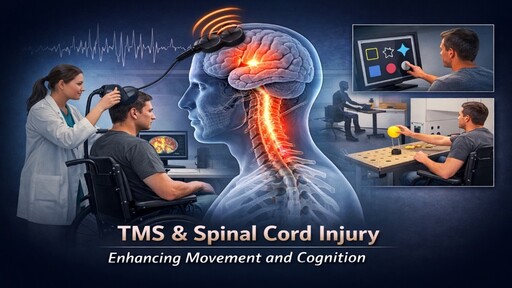
Brain stimulation and Recovery After Spinal Cord Injury
Pairing Brain and Peripheral Stimulation to Improve Recovery After Spinal Cord Injury
Embodiment is not only about perception - it is also about action. After a spinal cord injury, communication between the brain and the body is disrupted and this affects not only movement, and the sense of control over one’s actions, but also the internal representation of the body.
This research investigates whether Paired-Associative Stimulation - a non-invasive brain stimulation technique - can enhance motor and neuropsychological recovery by strengthening neural pathways spared by the injury, and support the brain’s natural capacity for reorganisation. This work brings together theory and treatment: understanding how the brain predicts, perceives and controls movement, and using that knowledge to improve rehabilitation outcomes.