
Brachial plexus injury

This is an investigation into brachial plexus injury and will initially focus on an arm support, however it is not expected that this will be the primary outcome. I will use the arm support as a design project to gain a deeper understanding of the condition. The learning gained from this initial investigation will provide a direction for further research.
The brachial plexus connects the spinal cord within the neck to the shoulder, they are a set of five large nerves that transmit the electrical signals for movement and feeling from the brain to the muscles within the shoulder. If damage occurs at any point along these 5 nerve roots, the signals from the brain do not reach the arm muscles and therefore prevent movement.
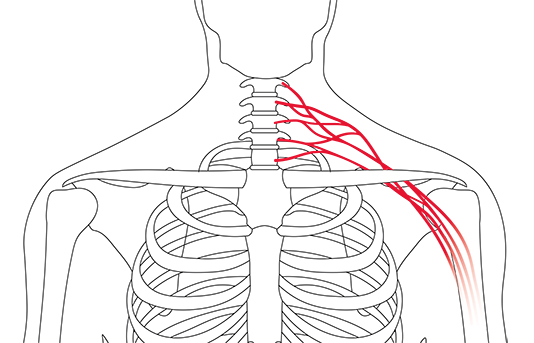
Injury to the brachial plexus commonly occurs through road traffic accidents, an impact forces the nerves to become over stretched.
The extent of the injury can vary in severity:
- Neurapraxia: Minimal nerve injury causing temporary symptoms, complete motor loss but quick recovery expected without intervention or surgery.
- Axonotmesis: A more severe stretch than neuropraxia, complete motor loss occurs but recovery is possible over an extended period.
- Neurotmesis: Severe nerve injury, complete recovery is impossible and surgical intervention is required.
The needs of individuals with BPI vary depending on the severity of the injury, support may be required for the following singularly or in combination, the shoulder, upper arm, elbow, wrist and fingers. A range of arm slings and splints are already available and some research has already been done in this area, however these are functional and usually unattractive products designed to provide simple arm support or subluxation of the shoulder or arm joint but do not consider the patients broader symptoms or personal requirements. My aim is to extend the function of the simple arm support and will consider multiple symptoms and combine them into one product. This is intended to be an additional utility for patients and not a replacement of existing medical treatment of symptoms.
This first stage focuses on the most severe form, neurotmesis and centres around a participant with permanent paralysis of the left arm after a motorcycle accident.
Summary of initial findings, symptoms and considerations stated by the participant during interview:
- Subluxation of the shoulder or arm joint.
- Poor posture, compensating for paralysed arm whilst sitting or carrying.
- Pain, this affects most adult patients and is often worse in an individual who has no prospect of recovery.
- Mental health, acceptance of condition and confidence in public and social situations.
- Overuse of unaffected limb requiring life style changes for protection.
- Effects of ageing, lopsided gait.
- Muscle wastage of affected arm including the aesthetic.
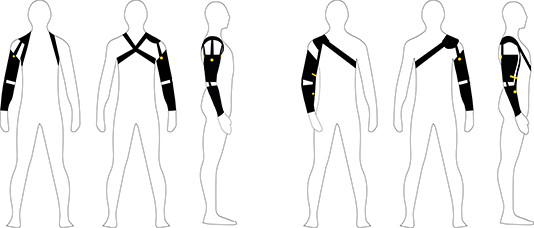
A common problem associated with BPI is subluxation of the shoulder joint, the choice of sling to attach the arm support to the body has been a primary factor in this study.
The participant is experiencing back and shoulder pain that stems from poor posture and the ‘dead weight’ of the affected arm, additionally he has muscle wastage and weight gain due to periods of inactivity and recuperation. The design includes two methods for attaching the arm support to the body for evaluation, for the purposes of this first stage of research I have utilised two existing slings.
The participant noted a need for control of his arm to prevent accidental damage to the skin including burns that can occur whilst undertaking simple chores. Paralysis of the arm and lack of feeling in the limb contribute to higher occurrence of accidental damage. The arm support is designed to protect the limb as it forms a protective hard cover over the skin and additionally provides the ability for repositioning.
His mental health and confidence has deteriorated, this is affecting every area of his life. The intent is to increase confidence in social situations, therefore it has been designed to be worn under clothing giving him confidence that his disability is hidden when he requires it, the repositionable function will allow a more natural body / arm positon when standing. As a contrary test, the arm support has also been designed to be worn visibly and has been styled to reflect his personality, it will be observed if this will in fact provide more confidence for him than hiding his injury, celebrating his difference and not conforming to what is considered normal. The design will additionally bulk up the profile of the arm to address muscle wastage, providing an improved aesthetic under clothing. The first trial of the arm support will continue over a 6 month period.

Helen Lansdown
Lecturer, (BA Hons) Model Design (Model Effects).